Ebola Symptoms
Ebola is one of those words that carries weight the moment it appears in a news headline. For most people, it conjures images from documentary footage, outbreak maps, and field hospitals in remote parts of Central and West Africa. But what Ebola does to the body, step by step, is far less understood than the fear surrounding it.
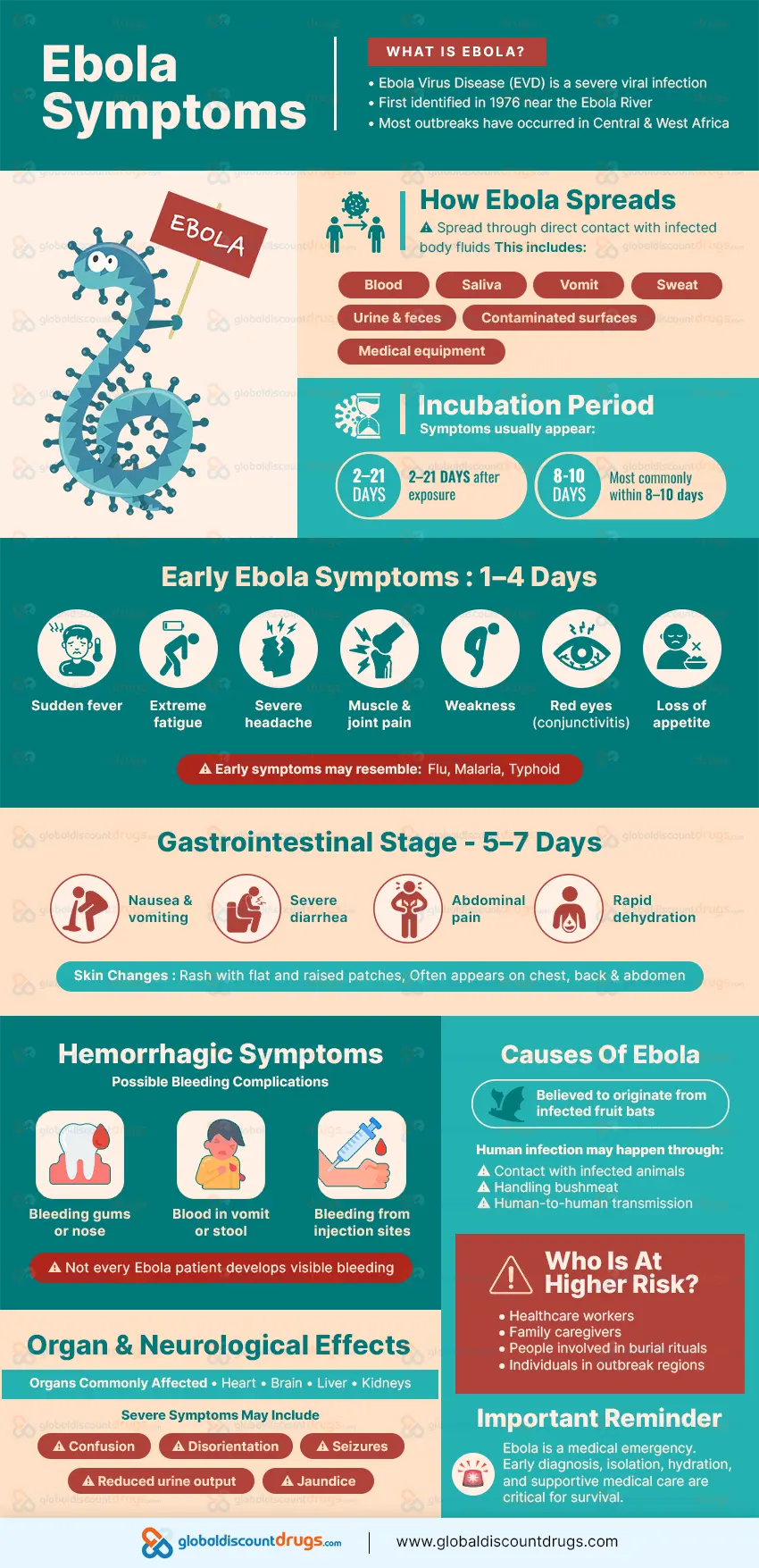
The disease is caused by a group of viruses belonging to the family Filoviridae. Ebola virus disease, or EVD, first appeared in 1976 near the Ebola River in what is now the Democratic Republic of Congo. Since then, multiple outbreaks have occurred across sub-Saharan Africa, with the 2014-2016 West African epidemic being the deadliest in recorded history.
Understanding Ebola symptoms matters. Not because the virus poses a realistic threat to most people reading this, but because health literacy helps communities respond when outbreaks occur. It also helps travelers, healthcare workers, and public health professionals recognize what the disease looks like before it reaches a critical stage.
This article walks through what Ebola does to the body, from the initial signs that resemble other illnesses to the more serious complications that define its progression.
 Patients may experience bleeding from the gums, nose, or injection sites. In more advanced cases, blood can appear in vomit or stool. Internal bleeding may also occur.
Studies conducted during the 2014-2016 epidemic found that visible hemorrhagic symptoms appeared in a smaller proportion of confirmed cases than many people assume. The name "Ebola hemorrhagic fever" gives the impression that bleeding is the defining feature, when in fact the earlier gastrointestinal and systemic symptoms are more consistent markers across cases.
Patients may experience bleeding from the gums, nose, or injection sites. In more advanced cases, blood can appear in vomit or stool. Internal bleeding may also occur.
Studies conducted during the 2014-2016 epidemic found that visible hemorrhagic symptoms appeared in a smaller proportion of confirmed cases than many people assume. The name "Ebola hemorrhagic fever" gives the impression that bleeding is the defining feature, when in fact the earlier gastrointestinal and systemic symptoms are more consistent markers across cases.
How Ebola Enters the Body
The Ebola virus spreads through direct contact with the blood or body fluids of a person who is sick. This includes saliva, sweat, vomit, urine, semen, and feces. The virus can also spread through contact with surfaces or objects contaminated with these fluids. A person is not contagious during the incubation period, which is the window between exposure and when symptoms first begin to appear. For Ebola, this period ranges from 2 to 21 days, though most people develop symptoms between 8 and 10 days after exposure. The virus enters the body through mucous membranes or breaks in the skin. Once inside, it targets specific immune cells and begins replicating at a pace the body is not prepared to manage.The First Signs: What Ebola Looks Like in the Opening Days
One of the more confusing aspects of Ebola is that its initial symptoms are not unique to the virus. The disease begins with a sudden onset of fever. Many patients also report fatigue, headache, muscle aches, and a general sense of feeling unwell. These early signs can resemble influenza, malaria, or typhoid fever. That overlap makes diagnosis harder in regions where multiple diseases circulate at once. Without laboratory testing, there is no reliable way to distinguish Ebola from other febrile illnesses in this first phase. Fever matters. It is often the first measurable sign. Within the first few days, a person may also develop a sore throat and joint pain. Some report a loss of appetite and marked weakness. At this point, nothing in the clinical picture points to Ebola with certainty.Days 1 to 4: The Initial Phase
Fever, fatigue, and muscle soreness dominate this window. Headaches can be severe. Some patients develop redness in the eyes, known as conjunctivitis. The person may look and feel like they have a bad flu, which complicates recognition outside of clinical settings.Days 5 to 7: When Gastrointestinal Symptoms Take Over
Around the fifth day, gastrointestinal symptoms tend to arrive. Nausea, vomiting, diarrhea, and abdominal pain become prominent. These symptoms can be intense and lead to substantial fluid loss in a short period. Dehydration becomes a serious concern at this stage. Some patients also develop a rash around this time. It is described as maculopapular, meaning it appears as both flat and raised patches across the skin. The rash often spreads across the chest, back, and abdomen.Hemorrhagic Complications: The Stage Most People Associate With the Disease
Ebola has long been associated with bleeding. But hemorrhagic symptoms are not present in every case, and they tend to appear after the gastrointestinal phase, not at the beginning. The bleeding that occurs in Ebola is caused by the virus's effect on the body's coagulation system, the network of proteins and cells that control clotting. When this system is disrupted, blood loses its ability to clot where it should. The result can be bleeding from multiple sites.
Patients may experience bleeding from the gums, nose, or injection sites. In more advanced cases, blood can appear in vomit or stool. Internal bleeding may also occur.
Studies conducted during the 2014-2016 epidemic found that visible hemorrhagic symptoms appeared in a smaller proportion of confirmed cases than many people assume. The name "Ebola hemorrhagic fever" gives the impression that bleeding is the defining feature, when in fact the earlier gastrointestinal and systemic symptoms are more consistent markers across cases.
Neurological and Organ-Related Effects
As the infection advances, the virus can affect multiple organ systems. This wide involvement is what makes Ebola so dangerous without proper medical support. The kidneys and liver are among the organs most affected. Liver inflammation can raise bilirubin levels, causing jaundice in some patients. Kidney involvement can reduce urine output and affect fluid balance in ways that require active management. Neurological symptoms have been documented in a portion of cases. These include confusion, disorientation, and in severe cases, seizures. The mechanisms behind neurological involvement are still under investigation, though inflammation and the body's immune response appear to play a role. The heart can also be affected. Some research involving outbreak survivors identified cardiac abnormalities in the weeks following recovery.Causes and Contributing Factors
Ebola is caused by viruses in the genus Ebolavirus. Six known species exist within this genus. Four are known to cause disease in humans: Zaire ebolavirus, Sudan ebolavirus, Taï Forest ebolavirus, and Bundibugyo ebolavirus. Zaire ebolavirus has been responsible for the most severe and well-documented outbreaks. The natural reservoir host of the Ebola virus is believed to be fruit bats of the Pteropodidae family. The virus appears to circulate in bat populations without causing illness in the animals themselves. Human outbreaks often begin when a person comes into contact with an infected animal through hunting, handling, or consuming bushmeat. From that point, human-to-human transmission becomes the primary driver of an outbreak. Healthcare settings without adequate protective equipment can become sites of amplified spread. This was a significant factor in early outbreaks, where the reuse of unsterilized needles contributed to transmission chains.Risk Factors: Who Faces Greater Exposure
Ebola does not discriminate by age or sex when exposure occurs. But certain circumstances place people at measurably higher risk. Healthcare workers in outbreak regions face considerable exposure risk. Despite protective equipment, proximity to bodily fluids creates vulnerability during every patient interaction. During the 2014-2016 epidemic, thousands of healthcare workers were infected. Family members and caregivers of sick individuals are also at elevated risk. In many communities, care begins at home before a formal diagnosis is reached. This creates exposure before the nature of the illness is understood. Individuals involved in burial practices that include direct contact with the deceased face particular risk. In parts of West and Central Africa, traditional burial rituals involve washing and preparing the body. Because Ebola virus remains active in the body after death, this has contributed to transmission chains during outbreaks. People in geographic proximity to an active outbreak, especially those in rural areas near forests where animal-to-human transmission is more common, carry a higher baseline risk of initial exposure.Diagnosis: How Doctors Confirm Infection
Confirming Ebola requires laboratory testing. Because the early symptoms mirror so many other diseases, no diagnosis can be made on clinical presentation alone. The most reliable diagnostic method is reverse transcription polymerase chain reaction, known as RT-PCR. This test detects the genetic material of the virus in a blood sample and can identify infection in the early stage of illness, sometimes within the first three days of symptom onset. Other tests include antigen detection assays and enzyme-linked immunosorbent assays, called ELISA tests, which look for viral proteins or antibodies in the blood. Testing must occur under strict biosafety conditions. Samples from suspected Ebola cases require careful handling to prevent accidental exposure in the lab. In outbreak settings, mobile laboratory units have been deployed to enable faster diagnosis in the field. Speed of diagnosis matters not just for the individual patient, but for outbreak containment.Treatment: Where Things Stand Now
There is no single cure for Ebola, but the landscape has changed considerably over the past decade. Two antiviral treatments have received approval for use against Zaire ebolavirus. Atoltivimab/maftivimab/odesivimab, sold under the name Inmazeb, and ansuvimab-zykl, sold as Ebanga, are monoclonal antibody therapies that help neutralize the virus. Clinical trials conducted during the 2018-2020 Congo outbreak showed both treatments improved survival compared to earlier experimental options. Supportive care remains the foundation of treatment for all Ebola patients. This involves maintaining fluid balance through intravenous fluids, managing electrolytes, providing adequate nutrition, treating pain, and addressing secondary infections. Patients who receive consistent supportive care tend to have better outcomes. And vaccines have become part of the response toolkit as well. The rVSV-ZEBOV vaccine, known as Ervebo, received approval in 2019 and has been used in ring vaccination campaigns, targeting close contacts of confirmed cases to build a protective barrier around each outbreak. Early identification and isolation of infected individuals improves both individual and community outcomes. The sooner a patient enters a care setting with appropriate resources, the greater the chance of survival.Survival and Recovery
Case fatality rates for Ebola vary by outbreak and by the quality of care available. Zaire ebolavirus has been associated with fatality rates ranging from 25% to 90% in different outbreak settings. With modern supportive care and the availability of specific treatments, survival rates have improved. Survivors often face long-term health effects. These can include joint pain, muscle pain, eye problems, fatigue, and neurological difficulties. This collection of post-illness challenges is sometimes referred to as Post-Ebola Virus Disease Syndrome. Some survivors carry the virus in certain body compartments, including the eyes and semen, for an extended period after clinical recovery. Sexual transmission from male survivors has been documented in cases weeks or months after recovery, which is one reason that post-recovery monitoring remains part of established clinical protocols.Prevention and Outbreak Control
For people outside active outbreak zones, the risk of Ebola exposure is low. The virus does not spread through air, water, or food in the way that respiratory illnesses do. Prevention in outbreak regions focuses on several interconnected strategies.Barrier Nursing and Protective Equipment
Healthcare workers managing Ebola patients wear full protective gear including gloves, gowns, face shields or goggles, and respirators. Removing this equipment follows strict protocols to prevent self-contamination, because the removal process itself carries risk.Safe Burial Practices
Public health teams work with local communities to establish burial procedures that respect cultural traditions while reducing the risk of transmission. Trained burial teams handle the deceased while wearing appropriate protective gear.Contact Tracing
Identifying and monitoring everyone who had contact with a confirmed case is central to outbreak containment. Contacts are monitored for 21 days. If they develop symptoms, they can be isolated and tested without delay.Community Education
And this is where trust matters. When communities have access to clear, honest information, cooperation with public health measures tends to improve. Outbreak control is not just a medical challenge. It is a communication challenge.Nutrition and Physical Recovery
Patients recovering from Ebola often face real nutritional challenges. The gastrointestinal symptoms that accompany the disease, combined with the metabolic demands of fighting a severe infection, can leave survivors in a weakened state. Adequate hydration and caloric intake are prioritized during the acute phase of treatment. After recovery, a gradual return to normal food intake with attention to protein, vitamins, and minerals can support physical repair. Healthcare providers working with survivors generally assess nutritional status as part of follow-up care. This remains an area where the evidence base is still developing, but the clinical need is clear.When to Seek Medical Attention
Anyone who has been in an area with a known Ebola outbreak and develops fever, fatigue, headache, or muscle pain should contact a healthcare provider before going directly into a clinic or emergency room. Calling ahead allows the facility to prepare appropriate isolation measures. This is not about causing alarm. Most fevers in outbreak-affected areas are caused by malaria or other common infections. But when there is a plausible exposure history, the possibility of Ebola needs to be assessed through proper channels. For people with no exposure history and no travel to affected areas, Ebola is not a realistic concern. The symptoms, though serious in the context of the disease, are not unique enough to raise suspicion without an epidemiological connection.Common Myths About Ebola
Myth: Ebola spreads through the air It does not. The virus requires direct contact with the blood or body fluids of a person who is sick. Casual contact, shared air space, or being near someone in the incubation period does not lead to transmission. Myth: A person with Ebola is contagious before they feel sick This is not supported by the evidence from past outbreaks. A person becomes contagious when symptoms appear. Someone who has been exposed but feels well does not pose a transmission risk. Myth: Ebola always causes dramatic bleeding Hemorrhagic symptoms are not present in every case. The gastrointestinal and systemic symptoms are more consistent features of the disease, and some patients recover without visible bleeding at all. Myth: Ebola cannot be treated That was closer to accurate before the development of targeted antiviral therapies and vaccines. With access to appropriate care today, survival is achievable for many patients, particularly when treatment begins at an early stage. Myth: Ebola only matters in African nations The 2014-2016 epidemic demonstrated how air travel can carry cases far beyond the outbreak's origin. A small number of cases were diagnosed in the United States and Europe during that period. Global preparedness is now part of how public health institutions plan their responses.Frequently Asked Questions
What is the first symptom of Ebola?
Fever tends to be the first sign, though it arrives alongside fatigue, headache, and muscle pain in many cases. These initial symptoms are difficult to distinguish from other illnesses without laboratory testing.How long after exposure do Ebola symptoms appear?
The incubation period ranges from 2 to 21 days. Most people begin showing symptoms somewhere between 8 and 10 days after exposure.Can Ebola be cured today?
Two monoclonal antibody treatments have been approved for Zaire ebolavirus and showed effectiveness in clinical trials. Supportive care also plays a significant role in improving outcomes. No universal cure covers all Ebola species at this time.Is Ebola contagious before symptoms appear?
No. A person with Ebola is not contagious during the incubation period. Transmission requires direct contact with the bodily fluids of someone showing active symptoms.What happens to people who survive Ebola?
Many survivors experience ongoing health challenges, including joint pain, fatigue, vision problems, and neurological symptoms. Some carry the virus in certain body fluids for an extended period after recovery, which requires monitoring and specific precautions.Is there a vaccine for Ebola?
Yes. The rVSV-ZEBOV vaccine (Ervebo) has received regulatory approval and has been used in outbreak responses targeting Zaire ebolavirus. Research into vaccines for other Ebola species is ongoing.A Final Thought
Ebola is a serious disease, but understanding it does not require fear. The biology is complex, the symptoms are real, and the threat to affected communities is genuine. The advances in treatment and vaccine development made over the past decade represent meaningful progress, and that progress deserves recognition. For most readers, what matters is understanding the basic facts: how the virus spreads, what it looks like in a person who is sick, and how the medical response has changed. That kind of knowledge is useful whether you are a healthcare professional, a traveler, a student, or someone who wants to understand what they are hearing in the news. Ebola remains rare outside active outbreak settings. For communities where it does appear, accurate information is part of what makes an effective response possible.References
- World Health Organization. Ebola Virus Disease. WHO Fact Sheet. 2023. https://www.who.int/news-room/fact-sheets/detail/ebola-virus-disease
- Centers for Disease Control and Prevention. About Ebola Virus Disease. CDC. https://www.cdc.gov/vhf/ebola/about.html
- Chertow DS, Kleine C, Edwards JK, et al. Ebola virus disease in West Africa: clinical manifestations and management. New England Journal of Medicine. 2014;371(22):2054-2057.
- Mulangu S, Dodd LE, Davey RT Jr, et al. A randomized, controlled trial of Ebola virus disease therapeutics. New England Journal of Medicine. 2019;381(24):2293-2303.
- Henao-Restrepo AM, Camacho A, Longini IM, et al. Efficacy and effectiveness of an rVSV-vectored vaccine in preventing Ebola virus disease: final results from the Guinea ring vaccination trial. The Lancet. 2017;389(10068):505-518.
- Clark DV, Kibuuka H, Millard M, et al. Long-term sequelae after Ebola virus disease in Bundibugyo, Uganda: a retrospective cohort study. The Lancet Infectious Diseases. 2015;15(8):905-912.
- Christie A, Davies-Wayne GJ, Cordier-Lassalle T, et al. Possible sexual transmission of Ebola virus, Liberia, 2015. MMWR Morbidity and Mortality Weekly Report. 2015;64(17):479-481.
- Mayo Clinic. Ebola Virus and Marburg Virus. https://www.mayoclinic.org/diseases-conditions/ebola-virus/symptoms-causes/syc-20356258
- Johns Hopkins Medicine. Ebola Virus Disease. https://www.hopkinsmedicine.org/health/conditions-and-diseases/ebola-virus-disease
- Spengler JR, Ervin ED, Towner JS, Rollin PE, Nichol ST. Perspectives on West Africa Ebola virus disease outbreak, 2013-2016. Emerging Infectious Diseases. 2016;22(6):956-963.
- National Institute of Allergy and Infectious Diseases. Ebola Disease. NIH. https://www.niaid.nih.gov/diseases-conditions/ebola
Editorial Standards
Content published on Global Discount Drugs is reviewed by healthcare professionals and supported by credible medical sources. Read our Editorial Content Policy to learn more.
 Blog
Blog
